Many people are not familiar with the term "abdominal aneurysm," or its full name. An abdominal aortic aneurysm (AAA) is a pathological expansion in the abdominal aorta. The condition is usually asymptomatic and can be thought of as a "silent killer." According to Dr. Frank Levi, a senior vascular surgeon, the prevalence of this condition in people over 65 is between 2-12%. It is estimated that about a thousand people develop a life-threatening abdominal aneurysm every year. Still, only 60% of them receive preventive surgery when their aneurysm is diagnosed before it ruptures. If it does rupture, the risk of mortality is incredibly high, over 90%. Men over 65, current or former smokers, and those with first-degree relatives who have aortic aneurysms are all at risk.
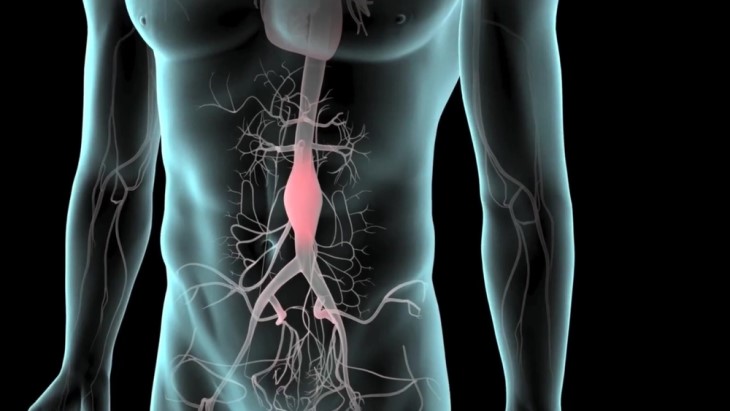
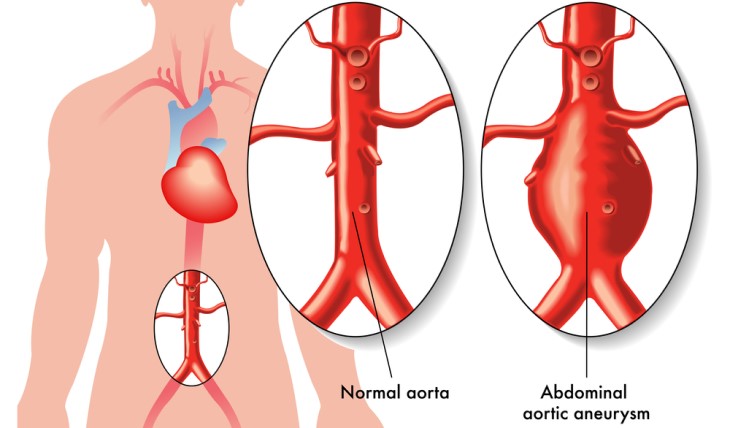
Before the 1950s, Dr. Levi explains, there was no reliable way to manage the illness. Today, the test is recommended to those aged 64 and up who have smoked in the past and/or currently, even if it was only in small amounts and for a short period, as well as to those with a close relative with the condition. Tobacco use and arteriosclerosis weaken the aorta wall, initiating an asymptomatic process where the artery, which usually measures 2-2.5 cm, starts to expand like a balloon, resulting in an aneurysm more than 3 cm in diameter. This process has been developing for years, "below the surface." One of the problems is that there are usually no symptoms.
The aorta expands slowly over many years. When it reaches a life-threatening diameter, a rupture may occur and then there is an immediate danger to life. "When the aneurysm ruptures, it leads to massive bleeding inside the body, and the person experiences abdominal pain and/or severe back pain accompanied by hemodynamic collapse (a state of shock/shaking, i.e. very low blood pressure) and usually loss of consciousness."
After that, there are two possibilities: the person succumbs to the bleeding in a few minutes, or the bleeding is contained, and they manage to get to a hospital. In fact, the only way to save their life is to perform emergency surgery to repair the aneurysm and stop the bleeding. "As long as the aneurysm is not repaired, the patient is in immediate danger throughout their life," said Dr. Levi. "It is important to note that even organizing this type of surgery and completing it is a complex matter and may take several hours." It is often the case that an abdominal aneurysm does not produce any symptoms.
This is why it is recommended to perform a screening if you're in a high-risk group. The test is non-invasive, quick, and painless, and it's done through abdominal ultrasound. If the test result reveals the diameter of the abdominal aorta to be over 3 cm, then it is considered an aneurysm, though mostly a small one that is not a major danger to the patient's life. Alternatively, a CT scan of the prostate or abdomen may be done.
The treatment is effective. When an aneurysm is identified via ultrasound or any other scan, the patient must be referred to a vascular surgeon for further review and to determine if treatment is needed. This is because many of the aneurysms are too small, do not require treatment, and only need a monitoring plan.
For men, an aneurysm with a size of 5.5 cm or more is an indication for treatment, while for women, the size must be 5 cm or greater as they usually have a slimmer aorta. A growth rate of 1 cm per year is another factor that might warrant treatment. If the aneurysm is smaller than that, the danger of it bursting is relatively low. Therefore, surgery may not be the best option due to the risks involved.

Nevertheless, these patients still need to have a follow-up plan for the aneurysm. Presently, when there is a requirement for an aneurysm to be treated, most operations are done with a minimally invasive approach as compared to the past when the surgery had higher chances of risks and complications. The procedure currently used is catheterization, wherein surgeons enter the vascular system through the arteries situated in the groin, navigate through the vascular system from the groin to the blood vessels in the abdomen and pelvis, and place a cloth-covered stent inside the blood vessels. This technique covers the entire aneurysmal area, and the blood flows beyond the stent, achieving a success rate of more than 95% with very low levels of complications, only a few percent.
In conclusion, the best course of action is to abstain from smoking or get regularly checked. The ultrasound test is quick, straightforward, non-intrusive, and poses no discomfort. The elective surgery to fix the aneurysm includes hospitalization, but generally, it goes well, and the patient can come back to their home and life after a brief period of time.